Development of a Reporting Guideline on Health Equity in Observational Research (STROBE-Equity)
Abstract
Cath Chamberlain,1 Peter Craig,2 Luis Gabriel Cuervo,3 Omar Dewidar,4 H. N. Ellingwood,5 Elizabeth Ghogomu,6 Billie-Jo Hardy,7 Tanya Horsley,8 Sonya Faber,9 Cindy Feng,10 Damian Francis,11 Sarah Funnell,12 Alison Krentel,9 Janet Jull,12 Elizabeth Kristjansson,13 Julian Little,9 Loveline Lum Niba,14 Tamara Kredo,15 Zack Marshall,16 Lawrence Mbuagbaw,17 Michael Johnson Mahande,18 Stuart Nicholls,19 Miriam Nkangu Nguilefem,9 Ekwaro Obuku,20 Oyekola Oloyede,21 Ebenezer Owusu-Addo,22 Kevin Pottie,23 Jacqueline Ramke,24 Alison Riddle,6 Anita Rizvi,13 Janet Hatcher Roberts,9 Larissa Shamseer,25 Melissa Sharp,26 Janice Tufte,27 Peter Tugwell,28 Xiaoqin Wang,29 Laura Weeks,30 Charles Wisonge,31 Luke Wolfenden,32 Taryn Young,33 Vivian Welch6
Objective
Advancing health equity requires improvements in the conduct, analysis, and reporting of health research. Many observational studies are relevant to health equity because they use data that can advance our understanding of health inequities, including the systemic structures that perpetuate them. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for the reporting of observational studies is highly endorsed by journal editors; however, the consideration of health equity has not been explicitly addressed in the STROBE statement. As a result, editors have been limited in their ability to promote the reporting of health equity data and considerations. The STROBE-Equity extension provides actionable guidance for equity-relevant observational studies to fill this gap.
Design
The development of STROBE-Equity adhered to a published protocol, informed by the Enhancing the Quality and Transparency of Health Research (EQUATOR) Network’s methodological framework including a scoping review of existing guidance, methods study, key informant interviews, and a global online survey. The project team was diverse across multiple domains, including lived experience of health inequity, gender, career stage, age, ethnicity, Indigenous background, disciplines, place of residence, and different decision-making roles. We recruited team members from our international network of patients, researchers, editors, and practitioners who had prior involvement in observational studies or expertise in reporting guidelines, biostatistics, knowledge translation, and patient engagement. We applied an integrated knowledge translation approach to (1) assess the reporting of health equity in published observational studies through a scoping review of available guidance, methodological review of observational studies, and key informant interviews; (2) seek wide international input on draft items; and (3) establish consensus amongst knowledge users and researchers through a 2-day consensus meeting. The development of the reporting guideline occurred between January 2020 and February 2024, with consensus achieved in May 2024.
Results
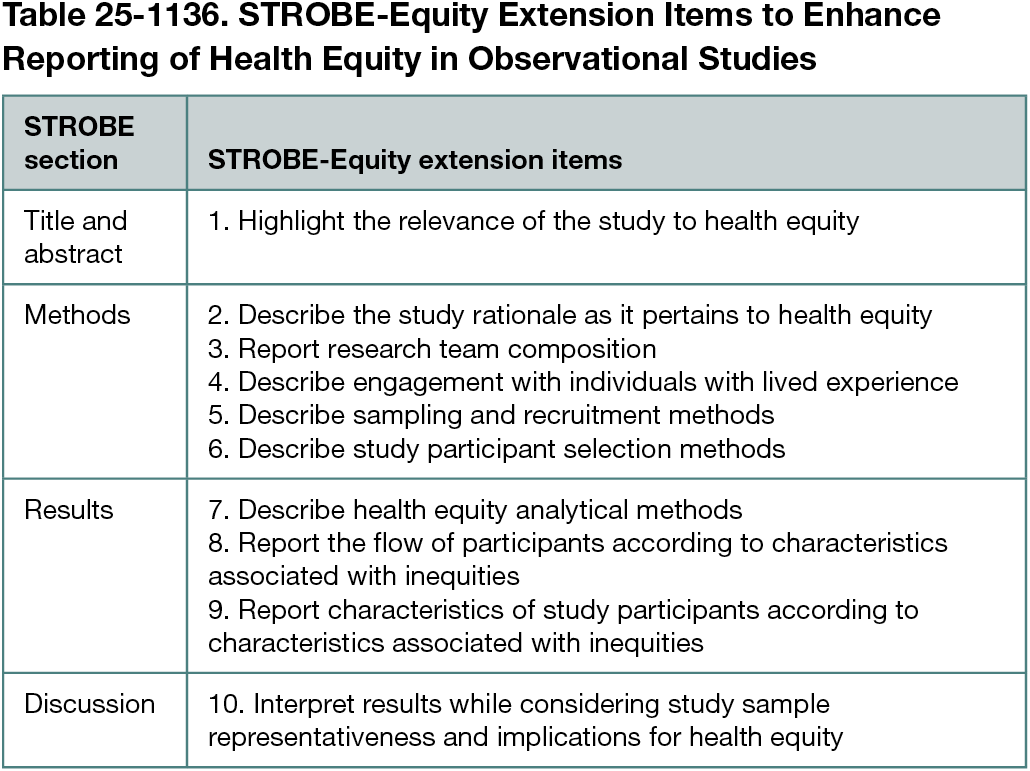
Our process identified 10 extension items for the STROBE statement to offer guidance for reporting of health equity (Table 25-1136). The items involve the following: (1) facilitating the identification of health equity relevance, (2) describing the purpose of the study in relation to health equity, (3) describing team composition, (4) engagement with individuals experiencing inequities relevant to the condition of interest, (5) sampling and recruitment of relevant populations, (6) participant selection, (7) analytical methods, (8) describing participant flow for relevant populations, (9) describing the characteristics of study participants, and (10) interpretation of study findings in relation to health equity.
Conclusions
The use of the STROBE-Equity extension alongside the original STROBE statement aims to promote transparent reporting of health equity data and considerations in observational research. Journal editors endorsing the use of this guideline can help advance health equity through improved reporting, ultimately contributing to research that informs more equitable policies and interventions.
1University of Melbourne, Australia; 2MRC/CSO Social and Public Health Sciences Unit, School of Health and Wellbeing, University of Glasgow, UK; 3Pan American Health Organization, Washington, DC, US; 4University of Toronto, Canada; 5Carleton University, Canada; 6Bruyère Health Research Institute, Canada; 7Dalla Lana School of Public Health, University of Toronto, Canada; 8Royal College of Physicians and Surgeons, Canada; 9School of Epidemiology and Public Health, University of Ottawa, Canada; 10Dalhousie University, Canada; 11PhD/School of Health and Human Performance, Center for Health and Social Issues, Georgia College, Milledgeville, GA, US; 12Queens University, Canada; 13School of Psychology, University of Ottawa, Canada; 14Department of Public Health, Faculty of Health Sciences, The University of Bamenda, Cameroon; 15South Africa Medical Research Council, South Africa; 16Department of Community Health Sciences, Cumming School of Medicine, University of Calgary and O’Brien Institute for Public Health, University of Calgary, Canada; 17McMaster University, Canada; 18Kilimanjaro Christian Medical Centre, Kenya; 19Centre for Practice-Changing Research, Ottawa Hospital Research Institute, Canada; 20Africa Centre for Systematic Reviews and Knowledge Translation, Kampala, Uganda; 21Sefako Makgatho Health Sciences University, South Africa; 22Bureau of Integrated Rural Development, College of Agriculture and Natural Resources, Ghana; 23Dalhousie University, Canada; 24International Centre for Eye Health, London School of Hygiene & Tropical Medicine, London, UK; 25Knowledge Translation Program, Li Ka Shing Knowledge Institute, Unity Health Toronto, Canada; 26Department of Public Health & Epidemiology, School of Population Health, Ireland; 27Catalyst for Positive Change, US; 28Department of Medicine, Faculty of Medicine, University of Ottawa, Canada; 29University of Ottawa Heart Institute, Canada; 30Canada’s Drug Agency, Ottawa, Canada; 31South Africa Medical Research Council, South Africa; 32University of Newcastle, Australia; 33Stellenbosch University, South Africa; vwelch@campbellcollaboration.org.
Conflict of Interest Disclosures
Kevin Pottie, Lawrence Mbuagbaw, Vivian Welch, and Peter Tugwell declare they are co-convenors of the Cochrane Health Equity Thematic Group. No other disclosures were reported.
Funding
This work was funded by the Canadian Institutes of Health Research. The funder had no role in the project design, implementation, or decision to publish. Vivian Welch is funded by a Public Health Agency of Canada and Canadian Institute of Health Research Applied Public Health Chair award. Kevin Pottie is funded by a Dalhousie University Faculty of Medicine Chair in Family Medicine.
Acknowledgment
The authors thank all the respondents to the global survey.